We first shared our framework approach 'for the assessment of Reduced-Risk Tobacco and Nicotine products' in 2015.[1] Over time, the presentation of our approach has evolved; however, the principles behind how our weight-of-evidence approach is used to assess our Smokeless Products have remained consistent.
We look to understand:

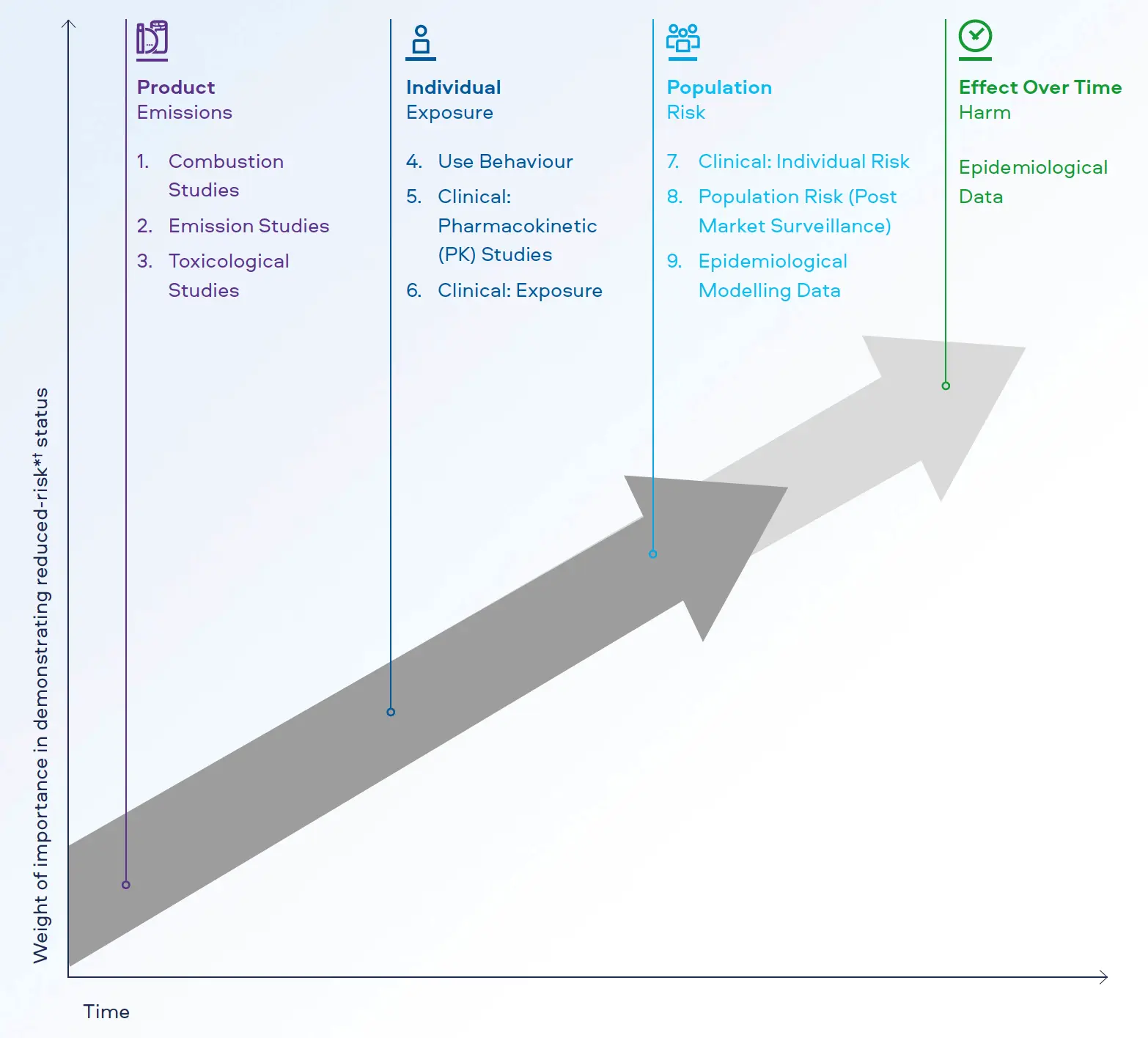
The original presentation of our 9-Step Scientific Risk Assessment Framework used the headings of Emissions, Exposure, Risk, and Harm. The evolution of this Framework now refers to these events as Product, Individual, Population, and Effect Over Time. We believe these titles better explain how the scientific evidence explores the Smokeless Products' effects at each assessment stage.
Dr Mark Forster
Principal Scientist, Global Life Sciences